")
")

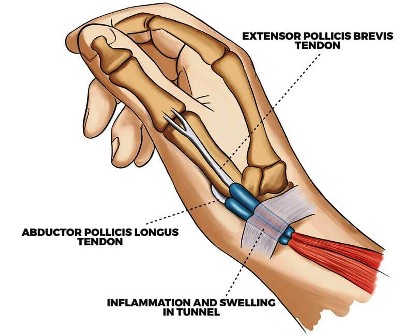 De Quervain’s tenosynovitis is one of the most common work-related upper limb musculoskeletal disorders especially in the age of smartphones, tablets and laptop devices. In 1895, Fritz de Quervain, a Swiss surgeon, first described tenosynovitis in a 35-year-old woman who had severe pain in the extensor muscle region of the thumb . It is a condition affecting the tendon sheaths of the abductor pollicis longus and the extensor pollicis brevis in the first dorsal compartment of the wrist. The thickening of the tendons sheaths develops at the point where the tendons pass in through the fibro-osseous tunnel located along the radial styloid at the distal wrist. Pain is exacerbated by thumb movement and radial and ulnar deviation of the wrist
De Quervain’s tenosynovitis is one of the most common work-related upper limb musculoskeletal disorders especially in the age of smartphones, tablets and laptop devices. In 1895, Fritz de Quervain, a Swiss surgeon, first described tenosynovitis in a 35-year-old woman who had severe pain in the extensor muscle region of the thumb . It is a condition affecting the tendon sheaths of the abductor pollicis longus and the extensor pollicis brevis in the first dorsal compartment of the wrist. The thickening of the tendons sheaths develops at the point where the tendons pass in through the fibro-osseous tunnel located along the radial styloid at the distal wrist. Pain is exacerbated by thumb movement and radial and ulnar deviation of the wrist
Epidemiology
The estimated prevalence of de Quervain tenosynovitis is about 0.5% in men and 1.3% in women with peak prevalence among those in their forties and fifties. Bilateral involvement is often reported in new mothers or child care providers .
Pathophysiology
The etiology of de Quervain’s tenosynovitis is not well understood. In the past, it was frequently attributed to occupational or repetitive activities involving postures that maintain the thumb in extension and abduction. As an example, it has been thought that new mothers are at risk postpartum due to repetitive motion of hands required to lift and hold newborns. Hormonal causes and fluid retention are another plausible explanation. The histopathology does not demonstrate inflammation but rather myxoid degeneration (disorganized collagen and increased cellular matrix) in patients referred for surgery.
Symptoms
- Pain and swelling in the ``anatomical''snuffbox.
- Pain radiating into the hand and forearm.
- Pain worsened by abduction and/or extension of the thumb.
Physical examination findings
- Tenderness at the ``anatomical'' snuffbox on palpation.
- Pain worsened by active abduction and/or extension of the thumb.
- Crepitus may be palpated along the radial forearm.
- Positive Finkelstein test.
Anastasios M. Margaritis
Occupational Health& Safety Specialist.
Bsc Physiotherapy & Sports Science.
Orthopaedic Manual Therapist.
Back Mechanic Specialist.
Differential diagnosis
Differential diagnosis of de quervain's tenosynovitis include :
- Intercarpal instabilities.
- Scaphoid fracture.
- Superficial radial neuritis (wartenberg's syndrome).
- C6 cervical radiculopathy.
- Osteoarthritis of 1 CMC.
Management options
- Worksite modification.
- Rest from aggravating movements.
- Anti-inflammatory and/or pain medication.
- Neutral wrist splinting with thumb spica.
- Physiotherapy.
- Corticosteroid injection.